External Apical Root Resorption (EARR) is a known risk of Orthodontic treatment. It has been studied since 1929 and is still poorly understood and unpredictable for individuals and even individual teeth for any individual. Root resorption can even take place in the absence of Orthodontic treatment. This does not help either patients or clinicians.
All of our patients are warned at the beginning of treatment in the information leaflets and specifically if they have root filled teeth, damaged teeth or habits. We also warn about nail biting.
The incidence in this practice is approximately 1:1000 – 4:5000. This is a low incidence but does not help if you are the 1:1000 affected.
Genetic factors, family factors, racial diversity, even speech patterns all seem to play a part. It is reported more in women than men. All of this simply goes to show that for any one individual resorption is unpredictable and the clinical picture is difficult to manage. If a tooth is lost the role of the Orthodontist is to make sure that the rest of the occlusion, whatever the starting position, allows a functional aesthetic restoration to be placed and that long term treatment management is secured for the patient.
External root resorption.
All precautions such as avoiding premolar extractions, headgear, facemasks, advice about habits, not using excessive forces on stainless steel wires are undertaken here.
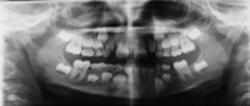
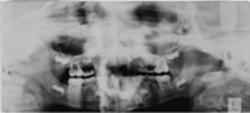
both front teeth had been traumatised and root filled but only one tooth showed external root resorption. In addition the guidance given about this is that if before treatment is commenced if it is suspected that resorption could be an issue then a repeat OPG is taken 6/12 after appliances are fitted. I have another example also in the lecture where the tooth had been completely traumatically avulsed, root filled outside of the mouth and reimplanted. I had to move this tooth later and no root resorption or discolouration took place. This is an extreme case and it should have resorbed but did not.
Internal root resorption:
Can mean there is an underlying genetic or medical problem. I have not seen a single case of Internal root resorption associated with orthodontic treatment. It appears to be a very rare condition and associated with Familial Bone dysplasias and McCune and Albright syndromes.
During the sixties and seventies the emphasis was on external root resorption, predisposing factors such as trauma and orthodontic treatment and most of the writers were Scandinavian (Linge and Linge, in particular). The work by Rygh, Reitan, Kvam and Lindhe has to a certain extent been superseded by the work done in recent years in cellular biology.
The key cellular factor seems to be iL1. This field is but still does not help individual patients affected.
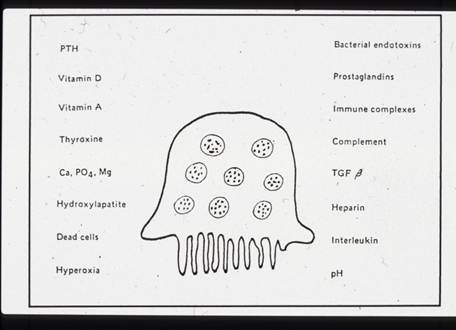
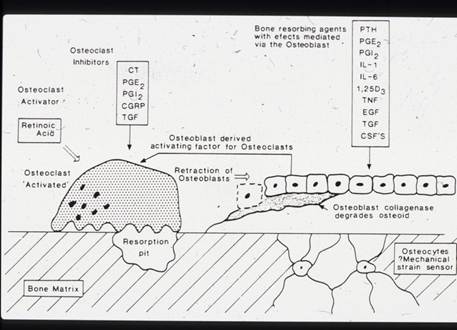
Slides showing some of the factors affecting Osteoclast differentiation and activation.
The emphasis now appears to be on the RANK/RANK L receptor ligand associated with Osteoprotegrin and TRAP positive cells inside the pulp. There also appears to be a distinction now between ODONTOCLASTS and OSTEOCLASTS.
J Orthod Sci. 2014 Oct-Dec; 3(4): 106–110.
PMCID: PMC4238077
Radiographic comparison of apical root resorption after orthodontic treatment between bidimensional and Roth straight-wire techniques
Khalid H Zawawi and Ghadah A Malki1
The field of orthodontics has been investigating the etiology of root resorption since 1927 when the relationship between orthodontic therapy and root resorption was recognized.[1,2] Unfortunately, even though this relationship has been known, little definitive conclusions have been reached as to the specific etiologic factors involved.[3] Brezniak addressed this issue when he noted that even though most root resorption studies attempt to determine the etiologic factors however, the causes remain obscure.[1,2]
The factors that have been proposed to induce root resorption are complex and include the following: Individual susceptibility, genetics, systemic factors, nutrition, chronological age, dental age, root shape, gender, history of resorption, previously traumatized teeth, endodontically treated teeth, density of alveolar bone, orthodontic therapy mechanics and duration of treatment.[1,4] This alludes to the difficulty in controlling confounding factors when performing a study. To help clarify this phenomenon much research has been performed to determine the process of root resorption during orthodontics.
1983 when Linge and Linge[10,11] standardized a magnification factor it was difficult to determine if the change in root length was a result of actual loss of tooth or positioning of the radiograph. Their method enabled the investigator to accurately compare root lengths of a pretreatment to a post treatment radiograph by measuring the crown length, factoring in that the crown length would not be affected by orthodontic therapy. The risk factors that lead to root resorption are vast and varied. To date it appears that much of this research is conflicting and generally inconclusive. One of the major untoward effects of orthodontic treatment is loss of root structure. Currently, the etiologic factors of root resorption are still unpredictable. Several factors have been investigated and proposed as risk factors for apical root resorption, including gender, age, systemic factors, morphological characteristics of the dentition, previous trauma, certain malocclusions, type of mechanics and type of tooth movement and forces used.[2,3,7,10,11,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35]
Several studies have also demonstrated a link between the technique used during fixed appliance orthodontic therapy and the amount of root resorption noted. However, the results were conflicting.[2,7,9,36,37,38]
The loss of root structure is a serious issue in orthodontic treatment however, it is important to note that most often the resultant loss is miniscule and does not affect the longevity of the teeth involved.[40] Accordingly, Remington found that mild to moderate shortening of the root length as a result of orthodontic therapy had no clinical significance.[5]
The etiology of root resorption is complex with a common occurrence during orthodontic treatment and the cause is difficult to identify. Furthermore, it is challenging to predict when root resorption will occur.
GENETIC FACTORS IN EXTERNAL APICAL ROOT RESORPTION AND ORTHODONTIC TREATMENT
1. 1Department of Oral Facial Development, Indiana University School of Dentistry, 1121 West Michigan Street, Indianapolis, IN 46202-5186, USA; and 2. 2Department of Medical and Molecular Genetics, Indiana University School of Medicine, Indianapolis, IN, USA;
- *corresponding author, jhartsfi@iupui.edu
Abstract
External apical root resorption (EARR) is a common sequela of orthodontic treatment, although it may also occur in the absence of orthodontic treatment. The degree and severity of EARR associated with orthodontic treatment are multifactorial, involving host and environmental factors. Genetic factors account for at least 50% of the variation in EARR. Variation in the Interleukin 1 beta gene in orthodontically treated individuals accounts for 15% of the variation in EARR. Historical and contemporary evidence implicates injury to the periodontal ligament and supporting structures at the site of root compression following the application of orthodontic force as the earliest event leading to EARR. Decreased IL-1β production in the case of IL-1B (+3953) allele 1 may result in relatively less catabolic bone modeling (resorption) at the cortical bone interface with the PDL, which may result in prolonged stress concentrated in the root of the tooth, triggering a cascade of fatigue-related events leading to root resorption. One mechanism of action for EARR may be mediated through impairment of alveolar resorption, resulting in prolonged stress and strain of the adjacent tooth root due to dynamic functional loads. Future estimation of susceptibility to EARR will likely require the analysis of a suite of genes, root morphology, skeleto-dental values, and the treatment method to be used—or essentially the amount of tooth movement planned for treatment.
(I) Introduction
Basic descriptors of root resorption are based on the anatomical region of occurrence—i.e., internal root resorption and external root resorption (cervical root resorption and external apical root resorption). Additional classification may involve two types of internal resorption: root canal (internal) replacement resorption and internal inflammatory resorption. External resorption can be classified into four categories according to its clinical and histologic manifestations: external surface resorption, external inflammatory root resorption, replacement resorption, and ankylosis. External inflammatory root resorption has been further categorized into cervical resorption with or without a vital pulp (invasive cervical root resorption) and external apical root resorption (EARR) (Ne et al., 1999).
This paper reviews EARR and its association with orthodontic treatment, and examines a new paradigm for its multifactorial etiology. EARR is a frequent iatrogenic outcome associated with orthodontic treatment, especially in the maxillary incisors, and may also occur in the absence of orthodontic treatment (Harris and Butler, 1992;Harris et al., 1993). Depending on the methodology, the incidence of EARR without orthodontic treatment has been reported to range from zero to 90.5% (Brezniak and Wasserstein, 1993). From 7% to 13% of individuals who have not had orthodontic treatment show some EARR on radiographs (Rudolph, 1936; Harris et al., 1993), presumably as a function of occlusal forces. There is an association of EARR in those who have not received orthodontic treatment with missing teeth, increased periodontal probing depths, and reduced crestal bone heights (Harris et al., 1993). Individuals with bruxism, chronic nail biting, and anterior open bites with concomitant tongue thrust may also show an increased extent of EARR before orthodontic treatment (Harris and Butler, 1992). Dental trauma, especially with re-implantation of an avulsed tooth, is also associated with increased EARR (Donaldson and Kinirons, 2001). For the most part, EARR is asymptomatic unless substantial tooth structure is affected, so early detection is unlikely unless radiographs are used (Brezniak and Wasserstein, 1993,2002b).
American Journal of Orthodontics.
May 2001Volume 119, Issue 5, Pages 511–515
Predicting and preventing root resorption: Part II. Treatment factors******
Glenn T. Sameshima, DDS, PhDa
Peter M. Sinclair, DDS, MSDb
Department of Orthodontics, University of Southern California, Los Angeles, Calif
Abstract
The main objective of this study was to determine which treatment factors are most clearly identified with external apical root resorption that is detectable on periapical radiographs at the end of orthodontic treatment. The records of 868 patients who completed fixed, edgewise treatment from experienced clinicians in private practice were examined. The horizontal and vertical displacement of the root apex of the maxillary central incisor was measured on cephalometric radiographs. Patients who underwent first premolar extraction therapy had more resorption than those patients who had no extractions or had only maxillary first premolars removed. Duration of treatment and the horizontal (but not vertical) displacement of the incisor apices were significantly associated with root resorption. No differences were found for slot size, archwire type, use of elastics, and types of expansion. However, there was considerable variation among the 6 offices that were surveyed; 1 office averaged nearly a full millimeter more of resorption per anterior tooth than the office with the least amount of root resorption. We conclude that the clinician should exercise caution with those patients in whom extraction therapy is planned for overjet correction that requires above average treatment time. Finally, each clinician should be aware that the root resorption seen in one practice may be different from the root resorption found in another practice. (Am J Orthod Dentofacial Orthop 2001;119:511-5)
THE ANGLE ORHODONTIST
Volume 72, Issue 2 (April 2002)
Review Articles
Orthodontically Induced Inflammatory Root Resorption. Part I: The Basic Science Aspects
Naphtali Brezniak, MD, DMD, MSDa and Atalia Wasserstein, DMDb
Naphtali Brezniak, MD, DMD, MSD, 3 Rav-Ashi St, No. 31, Tel-Aviv 69395, Israel (st@012.net.il)
| Abstract |
Orthodontically induced inflammatory root resorption (OIIRR) or, as it is better known, root resorption, is an unavoidable pathologic consequence of orthodontic tooth movement. It is a certain adverse effect of an otherwise predictable force application. Although it is rarely serious, it is a devastating event when it is radiographically recognized. Orthodontics is probably the only dental specialty that actually uses the inflammatory process as a means of solving functional and esthetic problems. Force application initiates a sequential cellular process. We know exactly how and when it is evoked, but we are unable to predict its actual overall outcome. The extent of this inflammatory process depends on many factors such as the virulence or aggressiveness of the different resorbing cells, as well as the vulnerability and sensitivity of the tissues involved. Individual variation and susceptibility, which are related to this process, remain beyond our understanding. We are therefore unable to predict the incidence and extent of OIIRR after force application. This contemporary review is divided into two parts. In Part I, we discuss the basic sciences aspects of OIIRR as a continuation of our previously published work. In Part II, we present the clinical aspects of this subject.
Keywords: Root resorption, Orthodontic treatment, Review
Accepted: October 2001; Final version received: May 2001;
Cited by
Yajun Hu, Wentao Liu, Zhijian Liu, Wenying Kuang and Hong He. (2015) Receptor activator of nuclear factor-kappa ligand, OPG, and IGF-I expression during orthodontically induced inflammatory root resorption in the recombinant human growth hormone–treated rats. The Angle Orthodontist 85:4, 562-569.
Online publication date: 3-Sep-2014.
Abstract | Full Text | PDF (3778 KB)
Naphtali Brezniak and Atalia Wasserstein. (2014) Defining and framing orthodontitis: A new term in orthodontics. The Angle Orthodontist 84:3, 568-569.
Online publication date: 21-Apr-2014.
Citation | Full Text | PDF (38 KB)
Henrik Lund, Kerstin Gröndahl, Ken Hansen and Hans-Göran Gröndahl. (2012) Apical root resorption during orthodontic treatment.The Angle Orthodontist 82:3, 480-487.
Online publication date: 16-Sep-2011.
Abstract | Full Text | PDF (380 KB)
Zhifeng Liu, Juan Xu, Lingling E and Dongsheng Wang. (2012) Ultrasound enhances the healing of orthodontically induced root resorption in rats. The Angle Orthodontist 82:1, 48-55.
Online publication date: 25-Jul-2011.
Abstract | Full Text | PDF (3000 KB)
Irin Sirisoontorn, Hitoshi Hotokezaka, Megumi Hashimoto, Carmen Gonzales, Suwannee Luppanapornlarp, M. Ali Darendeliler andNoriaki Yoshida. (2011) Tooth movement and root resorption; The effect of ovariectomy on orthodontic force application in rats. The Angle Orthodontist 81:4, 570-577.
Online publication date: 1-Mar-2011.
Abstract | Full Text | PDF (2082 KB)
Henrik Lund, Kerstin Gröndahl and Hans-Göran Gröndahl. (2010) Cone Beam Computed Tomography for Assessment of Root Length and Marginal Bone Level during Orthodontic Treatment. The Angle Orthodontist 80:3, 466-473.
Online publication date: 5-Jan-2010.
Abstract | Full Text | PDF (1047 KB)
Yeen Lim, Andrew Quick, Michael Swain and Peter Herbison. (2008) Temperature Effects on the Forces, Moments and Moment to Force Ratio of Nickel-Titanium and TMA Symmetrical T-loops. The Angle Orthodontist 78:6, 1035-1042.
Online publication date: 29-Jun-2009.
Abstract | Full Text | PDF (573 KB)
Mauricio A. Casa, Rolf M. Faltin, Kurt Faltin and Victor E. Arana-Chavez. (2006) Root Resorption on Torqued Human Premolars Shown by Tartrate-Resistant Acid Phosphatase Histochemistry and Transmission Electron Microscopy. The Angle Orthodontist 76:6, 1015-1021.
Online publication date: 15-Jul-2009.
Abstract | Full Text | PDF (703 KB)
Guangli Han, Shengfu Huang, Johannes W. Von den Hoff, Xianglong Zeng and Anne Marie Kuijpers-Jagtman. (2005) Root Resorption after Orthodontic Intrusion and Extrusion:. The Angle Orthodontist 75:6, 912-918.
Online publication date: 15-Jul-2009.
Abstract | Full Text | PDF (285 KB)
Naphtali Brezniak, Shay Goren, Ronen Zoizner, Ariel Dinbar, Arnon Arad, Atalia Wasserstein and Moshe Heller. (2004) A Comparison of Three Methods to Accurately Measure Root Length. The Angle Orthodontist 74:6, 786-791.
Online publication date: 15-Jul-2009.
Abstract | Full Text | PDF (184 KB)
Naphtali Brezniak, Shay Goren, Ronen Zoizner, Ariel Dinbar, Arnon Arad, Atalia Wasserstein and Moshe Heller. (2004) The Use of an Individual Jig in Measuring Tooth Length Changes. The Angle Orthodontist 74:6, 780-785.
Online publication date: 15-Jul-2009.
Abstract | Full Text | PDF (63 KB)
Internal root resorption
1992;47(4):54-75.
Lambrechts P, Vanhoorebeeck B.
Abstract
Root resorption can be divided into two main categories: internal root resorption and external root resorption. Internal root resorption is a pathology that can lead to tooth destruction in the short term and must consequently be stopped as soon as possible by applying adequate canal treatment. Until now, despite many research studies, very little is known about its causes and the way this kind of resorption appears. There are many different forms of external root resorption and it has a very diverse etiology. An external root resorption can thus appear in case of orthodontic treatment or due to the pressure brought by cysts, tumours or impacted teeth. A trauma or an infection may also lead to the development of an external root resorption. Because they are so diverse, each of these forms of external root resorption requires a specific treatment. It should also be noted that internal root resorptions, and some forms of external resorption too, often respond favourably to a calcium hydroxide treatment.
Aust Endod J. 2010 Aug;36(2):79-82.
Monozygotic twins with idiopathic internal root resorption: A case report.
1st Department of Stomatology, Faculty of Medicine, Pavol Jozef Safarik University, Kosice, Slovakia. danielurban@me.com
Abstract
This study presents the first case of internal root resorption in monozygotic twins. Genetic factors have been implicated in the development of root resorption lesions. The link between interleukin (IL)-1 gene polymorphism and root resorption had been reported. However, these studies have involved external root resorption. Twin healthy 17 year old Caucasian sisters were diagnosed with internal root resorption in their upper left central incisor. Neither had a history of orofacial trauma and neither had received orthodontic treatment. The presence of IL-1beta+C3953 allele is the sign of predisposed susceptibility to an exaggerated inflammatory response, including a limited feedback mechanism as a consequence of IL-1RN mutation. Most investigators agree that the listed polymorphism presents a significantly higher risk for development of pathological resorption. These were thought to be cases of true idiopathic resorption as none of the other factors related to root resorption was found.
Dent Traumatol. 2008 Oct;24(5):546-9.
Rapidly progressive internal root resorption: a case report.
Keinan D, Heling I, Stabholtz A, Moshonov J.
Department of Endodontics, The Hebrew University, Hadassah School of Dental Medicine, Jerusalem, Israel. dudinka99@yahoo.com
Abstract
The etiology of internal root resorption is not fully understandable, trauma and chronic pulpitis are considered the main risk factors. Usually the process is asymptomatic and diagnosed upon routine radiographic examination. This case report presents a rapid progression of internal resorption related directly to traumatic injury. A 16-year-old female arrived at the emergency room after a mild extrusion of the mandibular incisors. The initial treatment included repositioning and splinting of the teeth. Radiographs performed at repositioning and splinting demonstrated normal configuration of the incisor’s roots. Ten months later progressive internal resorption of the left mandibular first incisor was diagnosed. While treating this tooth similar process was detected in the right mandibular second incisor and in the mandibular left second incisor. The lower right first incisor reacted inconsistently to vitality test. As a result of the severe and rapidly progressive nature of the process, root canal treatments were performed in all lower incisors. The follow-up radiographs demonstrate arrest of the internal resorption process.
PMID: 18821960 [PubMed – indexed for MEDLINE]
Root resorption–diagnosis, classification and treatment choices based on stimulation factors.
Department of Endodontology, Tel Aviv University, Tel Aviv, Israel. fuss@netvision.net.il
Abstract
Etiology of different types of root resorption requires two phases: mechanical or chemical injury to the protective tissues and stimulation by infection or pressure. Injury can be similar in various types of root resorption. The selection of proper treatment is related to the stimulation factors. Intrapulpal infection is the stimulation factor in internal root resorption and external periradicular inflammatory root resorption. Adequate root canal treatment controls intrapulpal bacteria and arrests the resorption process. In cervical root resorption, infection originates from the periodontal sulcus and stimulates the pathological process. As adequate infection control in the sulcus is unlikely, removal of granulation tissue from the resorption lacuna and sealing are necessary for repair. Removal of the stimulation factor, i.e. pressure, is the treatment of choice in root resorption related to pressure during orthodontic treatment, or an impacted tooth or tumor. In ankylotic root resorption, there is no known stimulation factor; thus, no predictable treatment can be suggested. Therefore, various types of root resorptions can be classified according to the stimulation factors: pulpal infection resorption, periodontal infection resorption, orthodontic pressure resorption, impacted tooth or tumor pressure resorption, and ankylotic resorption.
Northwest Dent. 2010 May-Jun;89(3):45-7.
Causes and treatment of root resorption.
Department of Restorative Sciences, Division of Operative Dentistry, University of Minnesota School of Dentistry, Minneapolis, Minnesota, USA. larso004@umn.edu
Abstract
This article will review what is known about the classification, causes, and treatment of root resorptions that are either internal or external.
Int Endod J. 1999 Sep;32(5):343-60.
Endodontic-orthodontic relationships: a review of integrated treatment planning challenges.
Department of Restorative Sciences, Texas A & M University Health Science Center, Baylor College of Dentistry, Dallas 75246, USA.
Abstract
Literature review There is a paucity of information on the concise relationship between endodontics and orthodontics during treatment planning decisions. This relationship ranges from effects on the pulp from orthodontic treatment and the potential for resorption during tooth movement, to the clinical management of teeth requiring integrated endodontic and orthodontic treatment. This paper reviews the literature based on the definition of endodontics and the scope of endodontic practice as they relate to common orthodontic-endodontic treatment planning challenges. Literature data bases were accessed with a focus on orthodontic tooth movement and its impact on the viability of the dental pulp; its impact on root resorption in teeth with vital pulps and teeth with previous root canal treatment; the ability to move orthodontically teeth that were endodontically treated versus nonendodontically treated; the role of previous tooth trauma; the ability to move teeth orthodontically that have been subjected to endodontic surgery; the role of orthodontic treatment in the provision for and prognosis of endodontic treatment; and, the integrated role of orthodontics and endodontics in treatment planning tooth retention. Orthodontic tooth movement can cause degenerative and/or inflammatory responses in the dental pulp of teeth with completed apical formation. The impact of the tooth movement on the pulp is focused primarily on the neurovascular system, in which the release of specific neurotransmitters (neuropeptides) can influence both blood flow and cellular metabolism. The responses induced in these pulps may impact on the initiation and perpetuation of apical root remodelling or resorption during tooth movement. The incidence and severity of these changes may be influenced by previous or ongoing insults to the dental pulp, such as trauma or caries. Pulps in teeth with incomplete apical foramen, whilst not immune to adverse sequelae during tooth movement, have a reduced risk for these responses. Teeth with previous root canal treatment exhibit less propensity for apical root resorption during orthodontic tooth movement. Minimal resorptive/remodelling changes occur apically in teeth that are being moved orthodontically and that are well cleaned, shaped, and three-dimensionally obturated. This outcome would depend on the absence of coronal leakage or other avenues for bacterial ingress. A traumatized tooth can be moved orthodontically with minimal risk of resorption, provided the pulp has not been severely compromised (infected or necrotic). If there is evidence of pulpal demise, appropriate endodontic management is necessary prior to orthodontic treatment. If a previously traumatized tooth exhibits resorption, there is a greater chance that orthodontic tooth movement will enhance the resorptive process. If a tooth has been severely traumatized (intrusive luxation/avulsion) there may be a greater incidence of resorption with tooth movement. This can occur with or without previous endodontic treatment. Very little is known about the ability to move successfully teeth that have undergone periradicular surgical procedures. Likewise, little is known about the potential risks or sequelae involved in moving teeth that have had previous surgical intervention. Especially absent is the long-term prognosis of this type of treatment. During orthodontic tooth movement, the provision of endodontic treatment may be influenced by a number of factors, including but not limited to radiographic interpretation, accuracy of pulp testing, patient signs and symptoms, tooth isolation, access to the root canal, working length determination, and apical position of the canal obturation. Adjunctive orthodontic root extrusion and root separation are essential clinical procedures that will enhance the integrated treatment planning process of tooth retention in endodontic-orthodontic related cases.
Int Endod J. 2010 Aug;43(8):654-62. Epub 2010 Apr 23.
Study of external root resorption during orthodontic treatment in root filled teeth compared with their contralateral teeth with vital pulps.
Llamas-Carreras JM, Amarilla A, Solano E, Velasco-Ortega E, Rodríguez-Varo L, Segura-Egea JJ.
Department of Orthodontics, School of Dentistry, University of Seville, Seville, Spain.
Abstract
AIM: To determine whether root filled teeth and those with vital pulps exhibit a similar degree of external root resorption (ERR) as a consequence of orthodontic treatment.
METHODOLOGY: The study sample consisted of 77 patients, with a mean age of 32.7 +/- 10.7 years, who had one root filled tooth before completion of multiband/bracket orthodontic therapy for at least 1 year. For each patient, digital panoramic radiographs taken before and after orthodontic treatment were used to determine the proportion of external root resorption (PRR), defined as the ratio between the root resorption in the root filled tooth and that in its contralateral tooth with a vital pulp. The student’s t-test, anova and logistic regression analysis were used to determine statistical significance.
RESULTS: The mean PRR was 1.00 +/- 0.13, indicating that, in the total sample, there were no significant differences in root resorption in the root filled teeth and their contralateral teeth with vital pulps. Multivariate logistic regression analysis suggested that PRR was significantly greater in incisors (P = 0.0014; odds ratio = 6.2885, C.I. 95% = 2.0-19.4), compared to other teeth, and in women (P = 0.0255; odds ratio = 4.2, C.I. 95% = 1.2-14.6), compared to men.
CONCLUSIONS: There was no significant difference in the amount or severity of external root resorption during orthodontic movement between root filled teeth and their contralateral teeth with vital pulps.
PMID: 20456512 [PubMed – in process]
J Oral Sci. 2010;52(2):299-311.
Relation of soluble RANKL and osteoprotegerin levels in blood and gingival crevicular fluid to the degree of root resorption after orthodontic tooth movement.
Tyrovola JB, Perrea D, Halazonetis DJ, Dontas I, Vlachos IS, Makou M.
Department of Orthodontics, School of Dentistry, University of Athens, Greece. ioannatirovola@gmail.com
Abstract
The aim of the present study was the determination of the levels of osteoprotegerin and soluble RANKL in blood serum and in gingival crevicular fluid relative to the degree of orthodontic root resorption in a rat model. Blood samples and gingival crevicular fluid were collected from fourteen 6-month-old male Wistar rats weighing 350-500 g. A 25-g closed orthodontic coil spring was inserted between each upper right first molar and the upper incisors. After 21 days of loading, both upper first molars (treated and control) were extracted and studied under microcomputed tomography scanning. Statistical analysis demonstrated a positive linear correlation between the initial concentration of RANKL in blood serum and the degree of root resorption. The ratio of the initial concentrations of osteoprotegerin to RANKL in blood serum proved to be an independent prognostic factor of the degree of root resorption. The initial concentration of RANKL in gingival crevicular fluid showed a negative correlation to the initial concentration of RANKL in blood serum and for a finite range of initial concentrations of osteoprotegerin in gingival crevicular fluid, the dental root seemed protected against extreme external root resorption. Finally, the concentration of osteoprotegerin in blood serum decreased significantly in cases of severe root resorption.
British Journal of Orthodontics, Vol 12, 78-81, Copyright © 1985 by British Orthodontic Society
| ARTICLES |
Nailbiting: frequency and association with root resorption during orthodontic treatment
L Odenrick and V Brattstrom
The purpose of the present investigation was to determine the incidence andintensity of nailbiting and its possible role in root resorption duringorthodontic treatment. A sample of 1365 boys and girls, aged 13- 15 yearsold, were investigated about their nailbiting habits. The possible effectof nailbiting on root resorption during orthodontic treatment was evaluatedby radiographic examination of two groups, matched with regard to overjet,age, sex, length and type of orthodontic treatment with fixed orthodonticappliances, one group consisting of 21 severe nailbiters and the other agroup of 21 patients without the habit. Replies to questionnairesdistributed to 340 boys and girls showed that the incidence of nailbitingwas 45 per cent. The habit of severe nailbiting among 1025 of the childreninvestigated was registered in 14.3 per cent. There was no significantdifference regarding the habit between boys and girls. The apical root resorption index was significantly higher in the severe nailbiters before(p less than 0.01) and after (p less than 0.001) orthodontic treatment.
British Journal of Orthodontics, Vol 11, 155-157, Copyright © 1984 by British Orthodontic Society
J Clin Periodontol. 1991 May;18(5):330-6.
Periodontal tissue reactions to orthodontic extrusion. An experimental study in the dog.
Berglundh T, Marinello CP, Lindhe J, Thilander B, Liljenberg B.
Department of Periodontology, Faculty of Odontology, University of Gothenburg, Sweden.
Abstract
Orthodontic tooth extrusion is used at crown lengthening procedures or in conjunction with periodontal therapy aimed at eliminating or reducing angular bone defects. A technique for orthodontic extrusion combined with resection of the supracrestal attachment fibers (fiberotomy) was recently proposed as an adjunct to certain restorative procedures. The aim of the present investigation was to analyze reactions of the periodontal tissues to orthodontic extrusion when combined with fiberotomy. In 5 beagle dogs, the mesial roots of the 2nd, 3rd and 4th hemisected mandibular premolar were used as target roots while the distal roots served as reference units. After a baseline examination, an orthodontic extrusion device (stent) was installed and reactivated at 2-week intervals during an 8-week period of active tooth movement. Immediately following the installation of the stent and once every 2nd week, the target roots were exposed to fiberotomy. After the active period, the teeth were retained in their new position for a period of 8 weeks. Clinical, radiographical and histological measurements were performed. The results from the investigation demonstrated that orthodontic extrusion combined with supracrestal fiberotomy resulted in a coronal displacement of the tooth and was associated with pronounced recession of the gingival margin and extensive loss of connective tissue attachment. The degree of gingival recession and the amount of loss of connective tissue attachment were, however, less extensive than the amount of tooth extrusion. Thus, repeated fiberotomy obviously failed to entirely prevent coronal migration of the attachment apparatus. It was also observed that undesired attachment loss had occurred at the reference roots.
PMID: 2066448 [PubMed – indexed for MEDLINE]
Am J Orthod Dentofacial Orthop. 1990 Feb;97(2):130-4.
A comparison of apical root resorption during orthodontic treatment in endodontically treated and vital teeth.
Spurrier SW, Hall SH, Joondeph DR, Shapiro PA, Riedel RA.
School of Dentistry, University of Washington.
Abstract
The purpose of this study was to determine whether vital and endodontically treated incisors exhibit a similar severity of apical root resorption in response to orthodontic treatment. Forty-three patients who had one or more endodontically treated incisors before orthodontic treatment and who exhibited signs of apical root resorption after treatment were studied. In each patient the vital contralateral incisor served as a control. Vital incisors resorbed to a significantly greater degree than endodontically treated incisors (p less than or equal to 0.05). When patients were separated by gender, control teeth in males exhibited a statistically significant increase in resorption over control teeth in females. No significant differences were apparent between males and females when endodontically treated incisors were compared.
Eur J Orthod. 1988 Feb;10(1):30-8.
Evaluation of the risk of root resorption during orthodontic treatment: a study of upper incisors.
PMID: 3162877 [PubMed – indexed for MEDLINE]
Stomatologija. 2008;10(3):89-95.
Risk factors of root resorption after orthodontic treatment.
Orthodontic Clinic, Kaunas University of Medicine, Kaunas , Lithuania.
Abstract
External apical root resorption is an iatrogenic consequence of orthodontic treatment, although it may also occur in the absence of orthodontic treatment. Root resorption causes root shortening and breaks the integrity of teeth arch and this is very important for successful orthodontic treatment. Orthodontics is probably the only dental specialty that actually uses the inflammatory process as a means of solving functional and aesthetic problems. They should know the risk factors of root resorption and do everything to reduce the occurrence of root resorption. The aim of our review is to find, classify and estimate factors, that can initiate and induce root resorption during orthodontic treatment. The articles from 2002 to 2007 in English related to the topic were identified. Twenty four articles were selected for data collection. The severity and degree of root resorption associated with orthodontic treatment are multifactorial, involving host and environmental factors. The review shows that root resorption is significantly correlated with treatment duration, fixed appliance treatment, tooth structure, individual susceptibility, type of orthodontic tooth movement.
Linge L, Linge BO.
Am J Orthod Dentofacial Orthop. 1991 Jan;99(1):35-43.
Am J Orthod Dentofacial Orthop. 1991 Jan;99(1):35-43.
Patient characteristics and treatment variables associated with apical root resorption during orthodontic treatment.
Abstract
Multivariate analysis of patient characteristics and clinical variables was carried out with the maximum single maxillary incisor apical root resorption for each patient as the dependent variable. Root lengths were measured in standardized intraoral radiographs from 485 consecutively treated patients, 11.5 to 25 years of age. The correlation matrix revealed a complex pattern of positive and negative associations between the six pretreatment and seven treatment variables. Variables found to contribute significantly to apical root resorption were overjet, history of trauma to maxillary incisors before initiation of treatment, time of treatment with rectangular arch wires, time of treatment with Class II elastics, lip/tongue dysfunction, and/or history of finger-sucking habits persisting beyond the age of 7 years, and impacted maxillary canines to be corrected orthodontically. Clinical application of an open activator was significantly correlated with overjet but negatively correlated with apical root resorption, with the use of rectangular arch wires and/or Class II elastics, and with total banding time.
Stomatologija. 2008;10(3):89-95.
Risk factors of root resorption after orthodontic treatment.
Orthodontic Clinic, Kaunas University of Medicine, Kaunas , Lithuania.
Abstract
External apical root resorption is an iatrogenic consequence of orthodontic treatment, although it may also occur in the absence of orthodontic treatment. Root resorption causes root shortening and breaks the integrity of teeth arch and this is very important for successful orthodontic treatment. Orthodontics is probably the only dental specialty that actually uses the inflammatory process as a means of solving functional and aesthetic problems. They should know the risk factors of root resorption and do everything to reduce the occurrence of root resorption. The aim of our review is to find, classify and estimate factors, that can initiate and induce root resorption during orthodontic treatment. The articles from 2002 to 2007 in English related to the topic were identified. Twenty four articles were selected for data collection. The severity and degree of root resorption associated with orthodontic treatment are multifactorial, involving host and environmental factors. The review shows that root resorption is significantly correlated with treatment duration, fixed appliance treatment, tooth structure, individual susceptibility, type of orthodontic tooth movement.
Swed Dent J Suppl. 1995;105:1-45.
Orthodontic tooth movement and root resorption with special reference to force magnitude and duration. A clinical and histological investigation in adolescents.
Department of Orthodontics, Faculty of Odontology, Göteborg University, Sweden.
Abstract
The purpose of orthodontic treatment is to move teeth as efficiently as possible with least damage to teeth and their supporting tissues. Root resorption may occur as an unwanted side effect and may in some instances jeopardize an otherwise successful treatment. The general aim of this series of clinical investigations was to study the association between applied force, achieved tooth movement and related root resorptions. In 144 adolescents, the maxillary first or second premolar was buccally moved with a fixed orthodontic appliance. The variables studied were duration, magnitude and type of force. Moreover, both the occurrence of orthodontically induced root resorptions and the reparative potential were investigated in histological preparations of the teeth. When a continuous force of a clinically relevant magnitude (50 cN approximately 50 g) was applied, tooth movement increased gradually over time. Root resorptions were recorded in all test teeth but 4 (93%). After 3 weeks a few teeth revealed root resorptions extending half way to the pulp or more in the apical third of the root. No association was found between root resorptions and tooth movement. Doubling the force magnitude (100 cN approximately 100 g) affected neither the tooth movement nor the severity of root resorptions. However, when the force was increased 4 times (200 cN approximately 200 g), tooth movement increased 50% but still with no significant increase in the occurrence or severity of root resorptions. Tooth movement was achieved more efficiently with a continuous force than with an interrupted type of force of the same magnitude (50 cN). Root resorptions, though, did not seem to be affected differently by the two types of forces. Reduction of all types of applied forces was considerable, about 25-30%, already within one week. Repair with secondary cementum was recorded almost 3 times more often after 8 weeks (75%) of retention than after 1 week (28%). Irrespective of magnitude and type of force, large individual variations were observed regarding tooth movements and root resorptions as well as their reparative potential. The possible clinical consequences of the results obtained are discussed with regard to cost-benefit effects, convenience to the patient and risk of complications.
Int J Paediatr Dent. 2008 Mar;18(2):146-53.
Generalized idiopathic root resorption: a case report.
Eastman Dental Hospital, London, UK. nehanet20@hotmail.com
Abstract
BACKGROUND: Cases of generalized idiopathic root resorption have been reported in the literature. However the majority of previously reported cases have affected adults, and it has been rare that a possible link to a medical condition has been found.
CASE REPORT: The subject of this case report was 11 years old when generalized root resorption was first diagnosed. This case report is unusual in that the resorption may be connected to a bone dysplasia. The possible medical diagnoses and links to tooth resorption have been discussed for this very rare case.
CONCLUSION: The investigation into the exact diagnosis of the patient and the treatment of tooth resorption is still ongoing and has required input from many disciplines of Medicine and Dentistry.
1.
Rygh P.
Am J Orthod Dentofacial Orthop. 2001 Feb;119(2):196.
2.
[Incidence of tooth impaction in orthodontic treatment]
Reitan K.
1978 Jul-Aug;20(4):31-8.
3.
[Initial tissue behavior in changes of apical resorption]
Reitan K.
1974;6(3):194-211.
4.
Initial tissue behavior during apical root resorption.
Reitan K.
Angle Orthod. 1974 Jan;44(1):68-82.
5.
Ultrastructural changes in the periodontal ligament incident to orthodontic tooth movement.
Rygh P, Reitan K.
Trans Eur Orthod Soc. 1972:393-405.
6.
Comparative behavior of human and animal tissue during experimental tooth movement.
Reitan K, Kvam E.
Angle Orthod. 1971 Jan;41(1):1-14.
7.
Evaluation of orthodontic forces as related to histologic and mechanical factors.
Reitan K.
SSO Schweiz Monatsschr Zahnheilkd. 1970 May;80(5):579-96.
8.
Principles of retention and avoidance of posttreatment relapse.
Reitan K.
Am J Orthod. 1969 Jun;55(6):776-90. Review.
9.
Clinical and histologic observations on tooth movement during and after orthodontic treatment.
Reitan K.
Am J Orthod. 1967 Oct;53(10):721-45.
10.
Effects of hypercementosis on the movability of teeth during orthodontic treatment.
Humerfelt A, Reitan K.
Angle Orthod. 1966 Jul;36(3):179-89.
11.
[Histologic observations of practical importance in orthodontic treatment]
Reitan K.
1966 Apr;30(59):23-40.
12.
Humerfelt A, Reitan K.
Rep Congr Eur Orthod Soc. 1965;41:277-94.
13.
Behavior of Malassez’ epithelial rests during orthodontic tooth movement.
REITAN K.
Acta Odontol Scand. 1961 Dec;19:443-68.
14.
[Tissue changes caused by orthodontic apparatus.]
REITAN K.
1954 Oct 25;9(20):570-1.
15.
[Main factors in changes of supporting tissue in experimental tooth displacement.]
REITAN K.
1953 Dec 30;61(5):293-9.
16.
[Apposition and resorption processes in different types of bone tissue.]
REITAN K.
Nor Tannlaegeforen Tid. 1953 May;63(5):161-73.
17.
REITAN K.
Nor Tannlaegeforen Tid. 1953 Mar;63(3):65-77.
18.
REITAN K.
Acta Odontol Scand Suppl. 1951;6:1-240. Related citations
19.
[Balanced occlusion form the orthodontic viewpoint.]
REITAN K.
Suom Hammaslaak Toim. 1950 Mar;1:25-42.
J Clin Periodontol. 2002 Jun;29(6):580-5.
Cervical external root resorption in vital teeth.
Bergmans L, Van Cleynenbreugel J, Verbeken E, Wevers M, Van Meerbeek B, Lambrechts P.
Department of Operative Dentistry and Dental Materials, BIOMAT, Catholic University of Leuven, Belgium. Lars.Bergmans@med.kuleuven.ac.be
Abstract
External resorptions associated with inflammation in marginal tissues present a difficult clinical situation. Many times, lesions are misdiagnosed and confused with caries and internal resorptions. As a result inappropriate treatment is often initiated. This paper provides three-dimensional representations of cervical external resorption, based on X-ray microfocus-tomographical scanning of a case, which will aid the dental practitioner in recognizing characteristic features during clinical inspection. In addition, histopathological examination reveals the cellular morphology of the adjacent tissues.
Oral Dis. 2010 Jul 23. [Epub ahead of print]
Osteoclasts and odontoclasts: signaling pathways to development and disease.
Department of Orthodontics and Pediatric Dentistry, Medical School, University of Michigan, Ann Arbor, MI, USA.
Abstract
Oral Diseases (2010) doi: 10.1111/j.1601-0825.2010.01718.x Osteoclasts are cells essential for physiologic remodeling of bone and also play important physiologic and pathologic roles in the dentofacial complex. Osteoclasts and odontoclasts are necessary for tooth eruption yet result in dental compromise when associated with permanent tooth internal or external resorption. The determinants that separate their physiologic and pathologic roles are not well delineated. Clinical cases of primary eruption failure and root resorption are challenging to treat. Mineralized tissue resorbing cells undergo a fairly well characterized series of differentiation stages driven by transcriptional mediators. Signal transduction via cytokines and integrin-mediated events comprise the detailed pathways operative in osteo/odontoclastic cells and may provide insights to their targeted regulation. A better understanding of the unique aspects of osteoclastogenesis and osteo/odontoclast function will facilitate effective development of new therapeutic approaches. This review presents the clinical challenges and delves into the cellular and biochemical aspects of the unique cells responsible for resorption of mineralized tissues of the craniofacial complex.
J Oral Sci. 2007 Mar;49(1):1-12.
Physiologic root resorption in primary teeth: molecular and histological events.
Department of Orthodontics and Pediatric Dentistry, School of Dentistry, University of Louisville, KY 40292, USA. ehhaji01@louisville.edu
Abstract
Root resorption is a physiologic event for the primary teeth. It is still unclear whether odontoclasts, the cells which resorb the dental hard tissue, are different from the osteoclasts, the cells that resorb bone. Root resorption seems to be initiated and regulated by the stellate reticulum and the dental follicle of the underlying permanent tooth via the secretion of stimulatory molecules, i.e. cytokines and transcription factors. The primary root resorption process is regulated in a manner similar to bone remodeling, involving the same receptor ligand system known as RANK/RANKL (receptor activator of nuclear factor-kappa B/ RANK Ligand). Primary teeth without a permanent successor eventually exfoliate as well, but our current understanding on the underlying mechanism is slim. The literature is also vague on how resorption of the pulp and periodontal ligament of the primary teeth occurs. Knowledge on the mechanisms involved in the physiologic root resorption process may enable us to delay or even inhibit exfoliation of primary teeth in those cases that the permanent successor teeth are not present and thus preservation of the primary teeth is desirable.
Anat Rec. 2001 Dec 1;264(4):387-96.
Cellular events at the onset of physiological root resorption in rabbit deciduous teeth.
Department of Oral Histology, Matsumoto Dental University, Shiojiri, Nagano, Japan. sahara@po.mdu.ac.jp
Abstract
For elucidation of how physiological root resorption of deciduous teeth is initiated, the cellular events that occur surrounding the root of rabbit deciduous teeth before and at the onset of physiological root resorption were observed by means of light and electron microscopy. In addition, the cytodifferentiation of odontoclasts during the initial phase of this root resorption was evaluated by histochemical staining of tartrate-resistant acid phosphatase (TRAP) activity as a marker odontoclasts and their precursors. The present investigation was focused on the physiological root resorption of the deciduous lower second molar of rabbits from Day 0-5 postnatally. At birth, the deciduous molar had not erupted yet, and no TRAP-positive cell could be found surrounding the tissue adjacent to the root of the deciduous tooth. TRAP-positive mononuclear cells were initially detected in the coronal portion of the dental follicle of the permanent tooth at Day 1 postnatally. Ultrastructurally, these mononuclear cells had moderate numbers of mitochondria and short-strand rough endoplasmic reticulum, as well as scattered free ribosomes throughout their cytoplasm. TRAP-positive mononuclear cells then appeared in the cementoblast layer immediately adjacent to the surface of the deciduous roots. These mononuclear cells projected cytoplasmic extensions between the cementoblasts and made contact with the cementum. At that time, cell-cell contact was frequently observed between these mononuclear cells and cementoblasts. During 3-5 days postnatally, the number of TRAP-positive multinucleate odontoclasts on the root surface gradually increased. They had well-developed ruffled borders and made typical resorption lacunae on the root surface of the deciduous tooth. During this early postnatal period, neither inflammatory cells nor necrotic tissue could be observed surrounding the deciduous root. This study demonstrates that the dental follicle of the permanent tooth as well as the connective tissue adjacent to the deciduous root might play important role in site- and time-specific recruitment, development, and activation of odontoclasts before and at the onset of physiological root resorption.
J Morphol. 1999 Dec;242(3):295-309.
Microscopic and histochemical study of odontoclasts in physiologic resorption of teeth of the polyphyodont lizard, Liolaemus gravenhorsti.
Fuenzalida M, Illanes J, Lemus R, Guerrero A, Oyarzún A, Acuña O, Lemus D.
Laboratorio de Embriología Experimental, Programa de Morfología, ICBM, Facultad de Medicina, Universidad de Chile, Santiago, Chile. mfuenzal@machi.med.uchile.cl
Abstract
Using tartrate-resistant acid phosphatase (TRAP), we examined the cytodifferentiation of odontoclast cells in resorbing areas of dental tissues during the replacement of teeth in a polyphyodont lizard, Liolaemus gravenhorsti. We also report, by means of Lectin-HRP histochemistry, the distribution pattern of some specific sugar residues of TRAPase-positive cells. For detection of TRAPase activity, the azo dye-coupling technique was used. Lectin binding sites were demonstrated by means of specific HRP-lectins. The process of tooth resorption was divided into four stages: 1) preresorption-the wall of the dental pulp is covered with an odontoblast layer, and no TRAP-positive cells are in the dental pulp; 2) early resorption-TRAP-positive multinucleate odontoclasts are present on the dental wall, but the rest of the pulp surface is still covered with an odontoblast layer; 3) later resorption-the entire surface of the pulp chamber is lined with multinucleate odontoclasts; and 4) final resorption-the tooth has been totally resorbed. Odontoclasts are usually detached from the resorbed surface, and show signs of degeneration. Of the six lectins used, PNA, ECA, and UEA-1 bind to multinucleated but not mononuclear cells. All the remaining lectins, BS-1, RCA(120), and LTA showed no binding to any cells of the teeth. The significance of saccharidic moieties such as acetyl-galactosamine, acetyl-glucosamine, and fucose sugar residues is difficult to ascertain. Perhaps these oligosaccharides might be borne on molecules associated with odontoclastic resorption or associated with multinucleation of odontoclasts after attachment to the dentine surface.
Inhibition of RANK/RANKL signal transduction pathway: A promising approach for osteoporosis treatment
References and further reading may be available for this article. To view references and further reading you must purchase this article.
Yu-Di Baia, Fu-Sheng Yanga, Kun Xuana, Yu-Xiang Baib, , and Bu-Ling Wuc, ,
aDepartment of Paediatric Dentistry, School of Stomatology, Fourth Military Medical University, No. 145 West Changle Road, Xi’an 710032, China
bDepartment of Health Statistics, Fourth Military Medical University, No. 17 West Changle Road, Xi’an 710033, China
cDepartment of Operative Dentistry and Endodontics, School of Stomatology, Fourth Military Medical University, No. 145 West Changle Road, Xi’an 710032, China
Received 7 March 2008;
accepted 10 March 2008.
Available online 28 April 2008.
Summary
Osteoporosis is a bone disease causing impaired bone strength. It is characterized by increased osteoclast formation or enhanced bone resorption, leading to an increased risk of fragility fractures. Its prevalence increases with age. The advent of an aging population suggests that progressively more individuals will develop this disease in the aging population. A number of drugs for the prevention and treatment of osteoporosis act by inhibiting bone resorption. However, the effectiveness of osteoporosis treatment in clinical practice is limited. Since the osteoclast is the only cell in the body that is capable of resorbing bone, understanding its biology will be necessary for developing a new therapeutic approach for osteoporosis. Recently, it was discovered that the receptor activator of nuclear factor κB (RANK)/RANK ligand (RANKL)/osteoprotegerin (OPG) system is an important signal transduction pathway that regulates osteoclast formation. The binding of OPG to RANKL inhibits the binding between RANKL and RANK; this, in turn, prevents osteoclast precursors from differentiating and fusing to form mature osteoclasts. Therefore, the inhibition of the RANK/RANKL pathway inhibits osteoclast formation, differentiation, activation, and bone resorption. A potential clinical antiresorptive therapy can be developed by using an anti-RANKL monoclonal antibody, such as denosumab, that binds to RANKL with high affinity and specificity and blocks RANKL–RANK interactions.
1.
Silveira FF, Nunes E, Soares JA, Ferreira CL, Rotstein I.
Dent Traumatol. 2009 Jun;25(3):e43-7. Epub 2009 Feb 22.PMID: 19239482 [PubMed – indexed for MEDLINE]Related citations
2.
Invasive cervical resorption following trauma.
Heithersay GS.
Aust Endod J. 1999 Aug;25(2):79-85.PMID: 11411085 [PubMed – indexed for MEDLINE]Related citations
3.
Internal resorption complicating orthodontic tooth movement.
Brady J, Lewis DH.
Br J Orthod. 1984 Jul;11(3):155-7.PMID: 6591954 [PubMed – indexed for MEDLINE]Related citations
J Periodontal Res. 2009 Apr;44(2):248-57. Epub 2008 Oct 7.
Identifying early osteoclastic resorptive lesions in feline teeth: a model for understanding the origin of multiple idiopathic root resorption.
DeLaurier A, Boyde A, Jackson B, Horton MA, Price JS.
Source
Bone and Mineral Centre, Department of Medicine, University College London, UK. april@uoneuro.uoregon.edu
Abstract
BACKGROUND AND OBJECTIVE:
Domestic cats commonly suffer from external osteoclastic tooth resorption, a disease with many similarities to human multiple idiopathic root resorption. In both diseases, it is unclear whether anatomical features of the tooth surface are associated with a predisposition for resorptive lesions. The aim of the present study was to investigate the origin and progression of early feline osteoclastic resorptive lesions in teeth exhibiting no clinical signs of disease.
MATERIAL AND METHODS:
The entire surfaces of 138 teeth from 13 adult cats were analysed using back-scattered electron microscopy. The distribution of lesions was assessed by tooth type, location and between individuals.
RESULTS:
Seventy-three (53%) teeth showed at least one resorptive lesion. Eleven (85%) cats had lesions, and there was a significant association between increasing age and incidence of resorptive lesions. The highest frequency occurred in mandibular molars (82%). On average, there were 3.5 lesions per tooth. Fifty-two (38%) teeth featured resorptive lesions at the cemento-enamel junction. Twenty-three per cent of teeth with resorptive lesions showed evidence of repair of lesions that was limited to the root surface. There was no evidence of repair of resorptive lesions at the cemento-enamel junction.
CONCLUSION:
Resorption is prevalent without evidence of clinical disease, and occurred at younger ages than previously reported. It can initiate anywhere on the root surface, but lack of repair of lesions at the cemento-enamel junction indicates that mechanisms of replacement are absent or compromised in this region. Whereas resorption of the root may undergo repair, resorption at the cervix may progress to clinically evident lesions.

{kind=link}
A possible association between early apical resorption of primary teeth and ectodermal characteristics of the permanent dentition
+Author Affiliations1. Department of Orthodontics, School of Dentistry, University of Copenhagen, Denmark
- Address for correspondence Professor I. Kjær, Department of Orthodontics, School of Dentistry, University of Copenhagen, 20 Nørre Allé, DK 2200 Copenhagen N, Denmark, E-mail:ik@odont.ku.dk
Abstract
The hypothesis of this study is that children with unexpected early apical resorption of the primary teeth are also predisposed to resorption in the permanent dentition. Accordingly, the aim was to perform a longitudinal study focussing on the permanent teeth in children with unexpected early apical resorption in the primary dentition.
Panoramic radiographs of 12 children (7 boys and 5 girls) aged 6 years 4 months to 8 years 9 months with unexpected early apical resorption of primary teeth were identified from a dental archive of 588 patients. After written request, follow-up radiographs were obtained (2–15 year interval between early and follow-up radiographs). The radiographs were examined in order to verify the abnormal resorption pattern of the primary teeth and dental deviations in the permanent teeth, known to predispose for root resorption (i.e. invaginations, narrow crowns, abrupt root deflections, slender roots, short roots, taurodontia, agenesis, deviant pattern of eruption).
Primary dentition: Two phenotypically different resorption groups were identified: group I, eight patients (resorption of the roots only), and group II, four patients (resorption of root and crown). Permanent dentition: In all 12 children, dental deviations in the permanent dentition were observed. Additionally, idiopathic external apical resorption of the permanent teeth was seen in three children, two of whom had received orthodontic treatment.
Introduction
During orthodontic treatment, root resorption can be a complication. It is generally agreed that a tendency to root resorption is dependent on treatment factors and the patient’s individual susceptibility (Brezniak and Wasserstein, 1993; Hartsfield et al., 2004). Previous research has revealed that dentitions exhibiting certain morphological characteristics are predisposed to root resorption during orthodontic treatment (Kjær, 1995; Levander and Malmgren, 1988; Thongudomporn and Freer, 1998; Nishioka et al., 2006). In other studies, this association between resorption tendency and dental morphology was not observed (Lee et al., 1999; Kook et al., 2003; Mavragani et al., 2006).
A link has been demonstrated between resorption of the permanent teeth during orthodontic treatment and deviant resorption of primary teeth due to ectopic eruption of a permanent tooth and atypical external collum resorption (Kjær, 1995).
Kjær (1995) also showed a relationship between root resorption during orthodontic treatment and certain morphological characteristics and dental anomalies in the permanent dentition, such as invaginations, narrow crowns, short roots, slender roots, pipette-shaped roots, abrupt root deflections, taurodontia, agenesis, and ectopia.
Additionally, an association was seen between root resorption and anterior open bites as well as between root resorption and condylar changes such as flattening of the cranial contour of the mandibular condyle (Kjær, 1995).
The normal correlation between maturity stages of the permanent teeth and resorption stages of the corresponding primary teeth has been described byHaavikko (1973). Two abnormal apical resorption patterns in the primary dentitions have recently been described in 14 children (Bille et al., 2007). The abnormal resorption pattern was designated ‘unexpected early apical resorption’, and the subjects were divided into two groups according to phenotype. Group I was characterized by resorption of the roots only and group II by resorption of the entire root complex and partial resorption of the crown (Bille et al., 2007). The resorption pattern of group II was designated as teeth with a ‘shell appearance’.
In the present study, it was hypothesized that this recently described unexpected early apical resorption of the primary teeth observed in the presence of permanent successors also predisposes to root resorption of the permanent teeth during orthodontic treatment. The aim therefore was to determine whether children with unexpected early apical root resorption of the primary teeth in the later stage of dental development had deviations in the permanent dentition previously shown to be connected with root resorption (Kjær, 1995).
Material
Dental pantomograms of the early mixed dentitions for evaluating mainly the primary dentition
Dental pantomograms of 12 children (7 boys and 5 girls, aged from 6 years 4 months to 8 years 9 months) in the early mixed dentition were identified in an archive of dental radiographs. The archive consisted of radiographic material from 588 patients forwarded since 1995 from Danish municipal clinics to the Department of Orthodontics, Copenhagen School of Dentistry, for diagnostic guidance and treatment planning.
The criterion for identifying radiographs for the present study was the occurrence of a subjective estimate of unexpected early apical resorption of several primary teeth in regions with a permanent successor. In no case could the early resorption of several primary teeth be explained by caries, apical infection, or ectopic eruption of the permanent successor.
Follow-up radiographs for evaluating the permanent dentition
After a written request, follow-up radiographs were obtained (Table 1). These follow-up radiographs were taken 2–15 years after the radiographs of the early mixed dentition. Two of the 12 children had received orthodontic treatment during the follow-up period.
View this table:
Table 1
Overview of the radiographic material of children with unexpected early apical resorption of the primary teeth (early radiographs) and the findings of dental deviations in the permanent teeth in these children (follow-up radiographs)
Method
The radiographs were examined by two independent observers in order to verify the abnormal resorption pattern of the primary teeth and to divide the material into group I (abnormal root resorption only) and group II (abnormal root and crown resorption). Only radiographs with agreement between the observers were included. In the permanent dentition, dental deviations known to predispose for root resorption were registered, i.e. invaginations, narrow crowns, screwdriver-shape, abrupt root deflections, slender roots, short roots, taurodontia, agenesis, and deviant pattern of eruption (Kjær, 1995).
Invagination was defined as teeth with radiographically distinct enamel notching (a distinct cingulum dentis) according to Kjær (1995). A crown was defined as narrow when the diameter of the crown was no wider than the collum of the root. A root was defined as short if the root had the same size or appeared shorter than the crown, and a tooth was defined as taurodontic if the part of the tooth between the enamel dentine junction and the furcation was enlarged (Shaw, 1928).
Additionally, deviations from the normal eruption pattern of permanent teeth were noted, and resorption of permanent teeth was registered.
Results
Primary teeth
Two phenotypically different groups of resorption were identified according toBille et al. (2007). Eight children (four boys and four girls) belonged to group I (Figure 1) and four children (three boys and one girl) to group II (Figure 2).
View larger version:
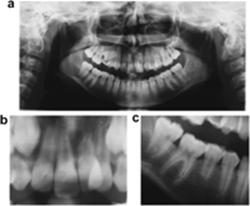
Figure 1
Dental pantomogram of a girl aged 6 years 4 months in the early mixed dentition with unexpected early apical resorption. Invaginations of the permanent maxillary lateral incisors, short roots of the permanent maxillary central incisors, and agenesis of the left permanent mandibular second premolar are seen. A follow-up radiograph (not shown) taken 2 years 8 months later confirmed findings of dental deviations seen on the first radiograph, but did not provide any additional findings of dental deviations in the permanent dentition.
View larger version:
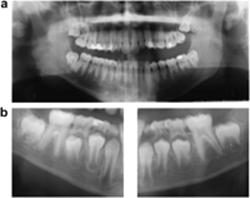
Figure 2
Dental pantomogram of a boy aged 8 years 9 months in the early mixed dentition with unexpected early apical resorption of the entire root complex and partial resorption of the crown of the primary maxillary second molars. Taurodontia is seen in the permanent maxillary first molars and agenesis of all second premolars. A follow-up radiograph (not shown) taken 3 years 8 months later confirmed the findings of dental deviations seen in the first radiograph. Additionally, the mandibular first premolars showed a deviant eruption pattern with resorption of the primary mandibular second molars.
Morphological characteristics of the permanent teeth
Dental deviations of the permanent teeth previously described by Kjær (1995) as associated with to root resorption during orthodontic treatment were seen in all 12 patients with unexpected early resorption of the primary teeth.
The following morphological characteristics and dental anomalies were seen in the subjects: invaginations in five (Figure 1), a narrow crown of the maxillary central or lateral incisors in one (not shown), abrupt root deflection of a maxillary incisor in one (Figure 3), slender or tapered roots in six (Figure 3), short roots in three (Figures 1 and 3), taurodontia in six (Figures 2 and 3), and agenesis in three (Figures 1 and 2). Pipette-shaped teeth were not registered.
View larger version:
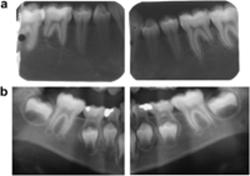
Figure 3
(a) Follow-up radiograph of the permanent dentition in a girl aged 11 years 6 months. Abrupt root deflection of the left maxillary central incisor, slender roots of the mandibular first molars, short roots of the second premolars and mandibular incisors, and taurodontia of the second molars. A deviant resorption pattern of the right primary maxillary second molar is seen. Dental pantomogram (DPT; not shown) of the early mixed dentition showed unexpected early apical resorption of the primary teeth. (b) Enlargement of the DPT of the girl shown in (a). Abrupt root deflection of the left maxillary central incisor is seen in (c). Enlargement of the right mandibular region of the DPT showing taurodontia of the second molar, slender roots of the first molar, and a short root of the second premolar.
Additional findings
Deviant eruption pattern of the permanent teeth.
Premature eruption of lower incisors was presumed in two subjects. Resorption of a neighbouring primary tooth during eruption of a permanent tooth was seen in six subjects, with resorption of a primary maxillary canine during eruption of a permanent maxillary lateral incisor as the most common type of deviant eruption pattern (Figure 1).
Resorption of permanent teeth.
Resorption of the permanent teeth was seen in four subjects. These resorptions were as follows: ongoing idiopathic external apical resorption of the mandibular first molars with the most pronounced resorption of the distal roots, seen in one patient who had not received orthodontic treatment (Figure 4); one case of internal crown resorption of a permanent molar; external apical resorption of molars, incisors, and lower canines, seen in two subjects who had received orthodontic treatment (Figure 5).
View larger version:
Figure 4
(a) Dental pantomogram (DPT) of the permanent mandibular regions of a girl aged 15 years 11 months showing short roots of the permanent mandibular first molars. The girl had not received orthodontic treatment. (b) For comparison of the mandibular regions (shown in (a)), two segments of the DPT of the early mixed dentition taken 9 years 5 months earlier of the same girl are shown. The root length of the first permanent molar appears longer than shown in (a), and accordingly an unexpected root resorption of the permanent mandibular molars has occurred. Unexpected early apical resorption of primary mandibular molars is also seen in (b).
View larger version:
Figure 5
(a) Dental pantomogram (DPT) of the permanent dentition of a boy aged 17 years 5 months with invaginations of the lateral incisors and short roots of mandibular molars. (b) For comparison of the mandibular regions (shown in (a)), two segments of a DPT of the same boy taken 9 years 3 months earlier are shown. Root resorption of the permanent mandibular molars has occurred since the DPT shown in (a) was taken. The patient has received orthodontic treatment. Note less severe early apical resorption of the primary teeth.
The distribution of dental deviations between the groups and genders is listed inTable 1.
Discussion
This longitudinal study examined the morphology of the permanent teeth on the radiographs of a sample of patients with unexpected early apical resorption of the primary teeth.
In the present study, the association between morphological deviations in the permanent teeth known to be of ectodermal origin and unexpected early apical resorption is described. This is the first communication suggesting that there is a connection between unexpected early apical resorption of the primary teeth and root resorption tendency of the permanent teeth, but further investigations as well as a longer follow-up period are needed in order to document this association.
The material in the present study was forwarded from different municipal dental clinics in Denmark. Although the radiographs varied in contrast and sharpness, they were considered suitable for the present investigation.
Two independent observers were used in this study in order to control and discuss the subjective evaluation of unexpected early apical resorption and morphological characteristics of permanent teeth. Although a subjective evaluation of tooth morphology on radiographs is not precise, it is a simple method that can easily be applied in dental practice with the purpose of identifying patients with root resorption tendencies.
The findings indicate that it is possible even in the early mixed dentition to identify patients particularly disposed to resorption of the permanent teeth. Very few studies have focussed on connections between resorption in the primary and the permanent dentitions (Kjær, 1995).
Several authors have shown a relationship between resorption of the permanent teeth and deviant morphology of the permanent teeth (Kjær, 1995; Levander and Malmgren, 1988; Thongudomporn and Freer, 1998; Nishioka et al., 2006), while others did not find an association (Lee et al., 1999; Kook et al., 2003; Mavraganiet al., 2006). Such disagreement might be due partly to different study designs as well as varied definitions of the morphological characteristics. For example,Thongudomporn and Freer (1998) did not find a connection between root resorption and taurodontia. In several studies, taurodontia is defined as the size and dimensions of the pulp chamber, which is often clearly visible on the radiographs (Shifman and Chanannel, 1978; Ruprecht et al., 1987). The problem is that the absence of a large pulp chamber does not prove the absence of taurodontia since the size of the pulp chamber in taurodontic teeth as well as in non-taurodontic teeth is gradually reduced with age and influenced by external stimuli. Other definitions of taurodontia exist based on different external measurements.
The main problem with regard to root resorption is that the mechanism initiating and controlling root resorption is not known. Recent studies of tooth resorption and tooth eruption have focussed on the cellular regulation of resorption processes. Especially RANK, RANKL, and OPG have been demonstrated in the roots of human primary teeth undergoing resorption (Lossdörfer et al., 2002) as well as in the permanent crown follicles of rats (Wise et al., 2002).
The present findings indicate that the molecular genetic factors responsible for resorption of the primary tooth roots are the same as those responsible for resorption of the permanent tooth roots at a later stage in development. This link between resorption in the primary and permanent dentition requires further elaboration.
In addition, the relationship between the resorption process and the ectodermal deviation in tooth morphology described in a previous study (Kjær, 1995) needs further elaboration. The connection between resorption and ectodermally derived deviations in morphology can only be understood if the resorption process is also dependent on ectodermal tissue. In a recent study, the epithelial rests of Malassez of ectodermal origin were documented as a continuous cell layer in the periodontal membrane (Becktor et al., 2007). If this ectodermal cell layer influences the resistance of the tooth root against resorption or the susceptibility to resorption, the relationship between morphology and resorption becomes understandable. Future studies will focus on the role of this epithelial cell layer of the periodontium during the resorption process.
Conclusions
Two types of unexpected early apical root resorption in the primary teeth were demonstrated in this study. In one type, the root was completely (severely) or partially (less severely) resorbed. The distinction between normal conditions and less severe resorption is difficult to define. In the other type of unexpected primary apical resorption, the root was completely resorbed and the crown partially resorbed. The present research did not comprise sufficient material to decide whether these two different phenotypic patterns of resorption are associated with different types of dental deviations in the permanent dentition. This is a condition that should be examined more closely as it is likely that the genetic causes for the two types of resorption could be different. Any gender differences should also be examined.
Once the different patterns and associations of root resorption are revealed at a macroscopic level, precautions can be taken to avoid resorption during orthodontic treatment and more systematic and goal-orientated research on the aetiology of resorption at a cellular and genetic level can be applied.
References
- Becktor KB,
- Nolting D,
- Becktor J,
- Kjær I
. Immunohistochemical localization of epithelial rests of Malassez in human periodontal membrane. European Journal of Orthodontics 2007;29:350-353.
- Bille MLB,
- Nolting D,
- Kvetny MJ,
- Kjær I
. Unexpected apical resorption of primary molars and canines. European Archives of Paediatric Dentistry 2007;8:144-149.
- Brezniak N,
- Wasserstein A
. Root resorption after orthodontic treatment: Parts 1 and 2. Literature review. American Journal of Orthodontics and Dentofacial Orthopedics1993;103:62-63. 138–146.
- Haavikko K
. Correlation between the root resorption of deciduous teeth and the formation of the corresponding permanent teeth. Proceedings of the Finnish Dental Society 1973;69:191-201.
- Hartsfield JK,
- Everett ET,
- Al-Qawasami RA
. Genetic factors in external apical root resorption and orthodontic treatment. Critical Reviews in Oral Biology and Medicine2004;15:115-122.
- Kjær I
. Morphological characteristics of dentitions developing excessive root resorption during orthodontic treatment. European Journal of Orthodontics1995;17:25-34.
- Kook Y-A,
- Park S,
- Sameshima GT
. Peg-shaped and small lateral incisors not at higher risk for root resorption. American Journal of Orthodontics and Dentofacial Orthopedics 2003;123:253-258.
- Lee RY,
- Årtun J,
- Alonzo TA
. Are dental anomalies risk factors for apical root resorption in orthodontic patients? American Journal of Orthodontics and Dentofacial Orthopedics 1999;116:187-195.
- Levander E,
- Malmgren O
. Evaluation of the risk of root resorption during orthodontic treatment: a study of upper incisors. European Journal of Orthodontics 1988;10:30-38.
- Lossdörfer S,
- Götz W,
- Jäger A
. Immunohistochemical localization of receptor activator of nuclear factor kappaB (RANK) and its ligand (RANKL) in human deciduous teeth. Calcified Tissue International 2002;71:45-52.
- Mavragani M,
- Apisariyakul J,
- Brudvik P,
- Selvig KA
. Is mild dental invagination a risk factor for apical root resorption in orthodontic patients? European Journal of Orthodontics 2006;28:307-312.
- Nishioka M,
- Ioi H,
- Nakata S,
- Naksima A,
- Counts A
. Root resorption and immune system factors in the Japanese. The Angle Orthodontist 2006;76:103-108.
- Ruprecht A,
- Batniji S,
- El-Neweihi E
. The incidence of taurodontism in dental patients. Oral Surgery, Oral Medicine, and Oral Pathology 1987;63:743-747.
- Shaw JCM
. Taurodont teeth in South African races. Journal of Anatomy1928;62:476-498.
- Shifman A,
- Chanannel I
. Prevalence of taurodotism found in radiographic dental examination of 1,200 young adult Israeli patients. Community Dentistry and Oral Epidemiology 1978;6:200-203.
- Thongudomporn U,
- Freer TJ
. Anomalous dental morphology and root resorption during orthodontic treatment: a pilot study. Australian Orthodontic Journal1998;15:162-167.
- Wise GE,
- Yao S,
- Zhang Q,
- Ren Y
. Inhibition of osteoclastogenesis by the secretion of osteoprotegerin in vitro by rat dental follicle cells and its implications for tooth eruption.Archives of Oral Biology 2002;47:247-254.
t Endod J. 2007 Jul;40(7):573-8.
Multiple idiopathic apical root resorption: a case report.
Source
Department of Endodontics, School of Dental Medicine, Shiraz University of Medical Sciences, Shiraz, Iran. fmoazzami@sums.ac.ir
Abstract
AIM:
To report a rare case of multiple idiopathic apical root resorption in an adult male.
SUMMARY:
A 27-year-old male with no history of medical or dental disorders was referred by his family dentist for evaluation of extreme root resorption involving the apical region of most of his teeth. A complete haematological investigation was conducted and all the results were within the normal range. Mobility of the teeth was physiologic and no abnormal periodontal pockets were observed. A diagnosis of multiple idiopathic apical root resorption was made.
KEY LEARNING POINTS:
*Apical root resorption of multiple teeth can be related to no specific aetiology and is known as idiopathic apical root resorption. *It is mostly seen in young adult males; maxillary teeth are more frequently involved. *No preventive or therapeutic regimen is known and monitoring accompanied by periodontal maintenance is recommended.
Bartley N, Türk T, Colak C, Elekdaq-Türk S, Jones A, Petocz P, et al. Physical properties of root cementum: Part 17. Root resorption after the application of 2.50 and 150 of buccal root torque for 4 weeks: a micro computed tomography study. Am J Orthod Dentofacial Orthop. 2011;139(4):e353-60.
Liou EJW, Chang PMH. Apical root resorption in orthodontics patients with en-masse maxillary anterior retraction and intrusion with miniscrews. Am J Orthod Dentofacial Orthop. 2010;137(2):207-12
Parker RJ, Harris EF. Directions of orthodontic tooth movements associated with external apical root resorption of the maxillary central incisor. Am J Orthod Dentofacial Orthop. 1998;114(6):677-83
Martins et al, 19 patients treated with intrusion mechanics combined with anterior retraction had statistically greater maxillary incisor root resorption than those treated with anterior retraction without intrusion. This finding is probably related to greater tooth movement necessary to close extraction spaces,8 , 27”
Duration of treatment has not been shown to be the sole cause of resorption. Many authors have in fact found the opposite.
- Artun J, Van’t Hullenaar R, Doppel D, Kuijpers-Jagtman AM. Identification of orthodontic patients at risk of severe apical root resorption. Am J Orthod Dentofacial Orthop. 2009;135(4):448-558.
- Mirabella AD, Artun J. Risk factors for apical root resorption of maxillary anterior teeth in adult orthodontic patients. Am J Orthod Dentofacial Orthop. 1995;108(1):48-55.
- Levander E, Malmgren O. Evaluation of the risk of root resorption during orthodontic treatment: a study of upper incisors. Eur J Orthod. 1988;10(1):30
- Martins DR, Tibola D, Janson G, Maria FR. Effects of intrusion combined with anterior retaction on apical root resorption. Eur J Orthod. 2012;34(2):170-5.
- Lim E, Sameshima G, Petocz P, Darendeliler A.Comparison of Australian and American orthodontic clinical approaches towards root resorption. Aust Orthod J. 2012;28(2):181-9.
Br Dent J
. 2018 Jun 22;224(12):937-943.
doi: 10.1038/sj.bdj.2018.441.
Hypophosphatasia and the importance of the general dental practitioner – a case series and discussion of upcoming treatments
C Feeney 1, N Stanford 2, S Lee 3, S Barry 1
Affiliations expand
- PMID: 29999027
Abstract
Hypophosphatasia (HPP) is an inherited metabolic disorder that results in poorly mineralised bones and teeth. Clinical symptoms vary widely from mild dental anomalies to fatal fetal defects. The most common dental symptoms include exfoliation of the primary incisors before the age of three with little or no root resorption, large pulp chambers, alveolar bone loss and thin dentinal walls. There is generally minimal periodontal inflammation associated with the bony destruction and tooth loss. The general dental practitioner is usually the first clinician to spot signs of the milder forms of HPP. Patients diagnosed with dental symptoms in childhood can go on to develop significant morbidity in middle age with chronic bone pain and stress fractures of the long bones. The primary dental care clinician is the key to early diagnosis of such cases, whether they present in childhood or adulthood. Emerging enzyme replacement therapy has considerably changed the landscape of the disease, resulting in astonishing improvements in bone mineralisation and a significant reduction in mortality and morbidity. It is increasingly likely that primary and secondary care clinicians will treat patients with the severe forms of HPP, who would previously not have survived infancy.
Similar articles
Plagmann HC, Kocher T, Kuhrau N, Caliebe A.J Clin Periodontol. 1994 Nov;21(10):710-6. doi: 10.1111/j.1600-051x.1994.tb00791.x.PMID: 7852617 Review.
Hughes SL, Parkes RC, Drage N, Collard M.Dent Update. 2017 Apr;44(4):317-8, 320-1. doi: 10.12968/denu.2017.44.4.317.PMID: 29172356
Okawa R, Matayoshi S, Kariya R, Ogaya Y, Nomura R, Nakano K.J Clin Pediatr Dent. 2020 Sep 1;44(5):348-351. doi: 10.17796/1053-4625-44.5.9.PMID: 33181846
Bloch-Zupan A, Vaysse F.Arch Pediatr. 2017 May;24(5S2):5S80-5S84. doi: 10.1016/S0929-693X(18)30020-4.PMID: 29405938 Review.
Ramer M, Basta R, Fisher K.N Y State Dent J. 1997 May;63(5):36-9.PMID: 9188264